- Joined
- Jun 20, 2011
- Messages
- 4,732
- Points
- 83
The Covid-19 Pandemic Does Not Exist
Introduction
There is much confusion and disinformation regarding the nature of the so-called Covid-19 “pandemic”.The definition of a pandemic is rarely mentioned by the governments and the corporate media.
What confirms the existence of a pandemic is not only the number of people affected by Covid-19, but also reliable evidence of a disease outbreak which is spreading over a wide geographic area “including multiple countries or continents”
“A pandemic is an epidemic that becomes very widespread and affects a whole region, a continent, or the world” (Nature)
The above definition does not in any way describe the alleged spread of SARS-CoV-2.
There Never Was a Pandemic
I have investigated this matter extensively since January 2020 and have come to the conclusion based on relevant definitions, the history of the corona crisis as well as the official WHO “estimates” of “Covid positive cases” that there never was a pandemic.At the outset of the corona crisis, the number of so-called confirmed positive cases was abysmally low, starting with 83 positive cases outside China (6.4 billion people). These ridiculously low numbers were nonetheless used to justify the launching on January 30th 2020 of a Worldwide Public Health Emergency leading up six weeks later to the official declaration of a Worldwide Pandemic on March 11, 2021 (44,279 covid positive cases outside of China).
Test, Test, Test
It was only in the wake of the official announcement of the pandemic (March 11, 2020) that the number of Covid-19 cases went fly high. And that had nothing to do with the alleged spread of the disease to major regions of the World.A highly organized Covid testing apparatus was established. The mandate was Test Test Test.
Meanwhile, the Gates Foundation together with other billionaire philanthropists generously funded sizeable investments in PCR-RT testing

Screenshot, Forbes, July 1, 2021
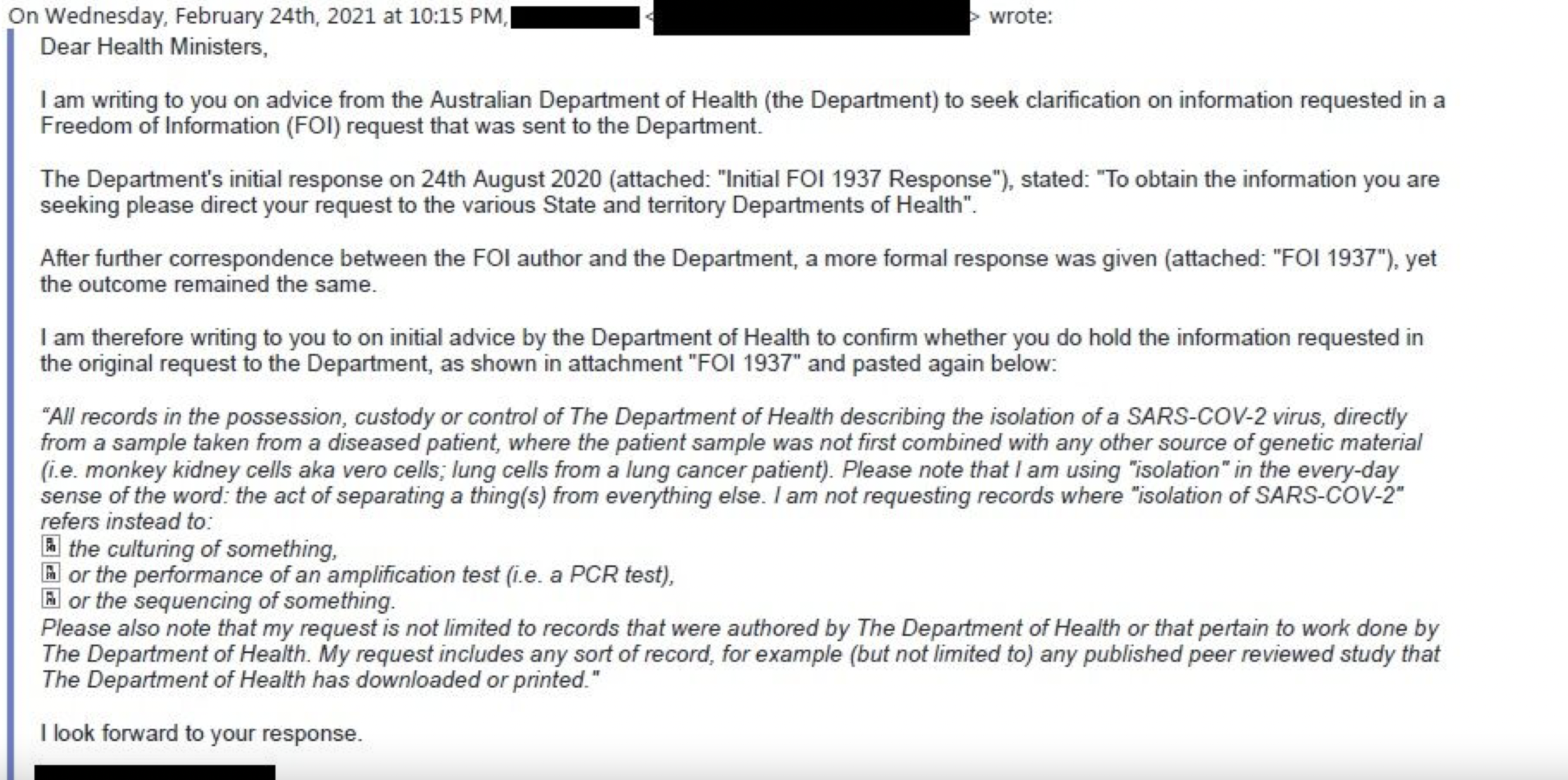
The Polymerase Chain Reaction Test (PCR-RT)
The “customized” and flawed PCR-RT Test (which does not under any circumstances identify the SARS-CoV-2 virus) has been used Worldwide to generate millions of erroneous Covid positive cases.The latter were then used to sustain the illusion that the alleged pandemic was Real and that the SARS-CoV-2 virus was spreading relentlessly to all major regions of the World.This assessment based on erroneous numbers was then used to spearhead the fear campaign.
Erroneous figures of positive cases are now part of a giant data base, coupled with fake data on so-called Covid-19 mortality.
In turn, these millions of positive cases are then used to justify every single Covid-19 related policy adopted since March 2020, including the lockdown, confinement of the labor force, social distancing, the facemask, the closure of schools, colleges and universities, the suspension of cultural and sports events, etc.
This tabulation of Covid positive cases was also used as a pretext to justify the March 2020 “closure” of the global economy (simultaneous “closure” of 190 national economies of member states of the United Nations) allegedly with a view to saving lives.
And since December 2020, the alleged “Covid-19 pandemic” is used to convince people Worldwide that the Covid-19 vaccine (coupled with the Vaccine Passport) is the “solution” to curbing the spread of the disease.
Defining the Pandemic
In analyzing the evolution of the Covid-19 crisis, we must distinguish between three important concepts: The Outbreak of the Disease, the Epidemic and the Pandemic.The Outbreak constitutes:
“a sudden rise in the incidence of a disease” and typically is confined to a localized area or a specific group of people. Should an outbreak become more severe, and less localized, it may be characterized as an epidemic. If it broadens still further, and affects a significant portion of the population, the disease may be characterized as a pandemic. Webster-Merriam
The Epidemic is defined as a disease outbreak:
“affecting or tending to affect a disproportionately large number of individuals within a population, community, or region at the same time”
The Pandemic is broadly defined as an extension of the epidemic:
“An outbreak of a disease occurring over a wide geographic area (such as multiple countries or continents) and typically affecting a significant proportion of the population” (Webster-Merriam, emphasis added)
Based on the above definitions, as well as data released by the Chinese health authorities pertaining to positive cases, there was an Outbreak of the Disease in Wuhan, Hubei Province in late December 2019.
A review of the data leading up to the official WHO decision to declare a Pandemic on March 11, 2020 confirms the following:
- no evidence of a pandemic, characterized by an outbreak of Covid-19 “over a wide geographic area such as multiple countries or continents”
- The official published data of the WHO pertaining to the alleged spread of Covid-19 do not confirm the existence of either an epidemic nor a pandemic.
The Public Health Emergency of International Concern (PHEIC)
The first step towards building a fake consensus on the potential spread of the disease was initiated on January 30, 2020 with the decision by the WHO to declare a Public Health Emergency of International Concern (PHEIC).Under the 2005 International Health Regulations (IHR), the member states of the WHO have “a legal duty to respond promptly to a PHEIC”.
Without a shred of evidence, the Director General of the WHO declared the PHEIC, pointing to
“a public health risk to other States through the international spread of disease and to potentially require a coordinated international response”.
This warning pointed to the possible occurrence of a pandemic.
A Global Health Emergency based on 83 Covid-19 Positive Cases Outside China
The January 30 2020 PHEIC intimates the possibility of a pandemic. In an advisory published on December 19, 2019 (barely two weeks before the Wuhan outbreak), the WHO reconfirmed the definition of the PHEIC:“a situation that is:
- serious, sudden, unusual or unexpected;
- carries implications for public health beyond the affected State’s national border;
- may require immediate international action.”
 The calling of a PHEIC was a fraudulent decision on the part of the WHO Director General Dr Tedros Adhanom Ghebreyesus. Why? Because on the 30th of January 2020 there were 83 Covid positive cases outside China for a population of 6.4 billion people.
The calling of a PHEIC was a fraudulent decision on the part of the WHO Director General Dr Tedros Adhanom Ghebreyesus. Why? Because on the 30th of January 2020 there were 83 Covid positive cases outside China for a population of 6.4 billion people.83 cases in 18 countries, and only 7 of them had no history of travel in China. (see WHO, January 30, 2020).
The “Evidence” Points to Fraud
There was nothing “serious, sudden, unusual or unexpected” requiring immediate international action. These ridiculously low numbers which were not mentioned by the media, did not prevent the launching of a Worldwide fear campaign.
These ridiculously low numbers which were not mentioned by the media, did not prevent the launching of a Worldwide fear campaign.In the week preceding this historic WHO decision. The PHEIC was the object of “consultations” at the World Economic Forum (WEF), Davos (January 21-24). The WHO Director General Dr. Tedros was present at Davos. Were these consultations instrumental in influencing the WHO’s historic decision to declare a PHEIC on January 30th.
Was there a Conflict of Interest as defined by the WHO? The WHO’s largest donor is the Bill and Melinda Gates Foundation, which together with the WEF and CEPI had already announced in Davos the development of a Covid-19 vaccine prior to the historic January 30th launching of the PHEIC.
The WHO Director General had the backing of the Bill and Melinda Gates Foundation, Big Pharma and the World Economic Forum (WEF). (See Michel Chossudovsky, E book, Chapter II)
“Divisions” Within the WHO
There are indications that the decision of the WHO Director General to declare a PHEIC was taken on the sidelines of the World Economic Forum (WEF) in Davos (January 21-24) overlapping with the Geneva January 22 meeting of the WHO emergency committee on 22 January, 2020. According to the minutes of this meeting (excerpt below), there were divisions within the Emergency Committee regarding the calling of a PHEIC:On 22 January, the members of the Emergency Committee expressed divergent views on whether this event constitutes a PHEIC or not. At that time, the advice was that the event did not constitute a PHEIC, but the Committee members agreed on the urgency of the situation and suggested that the Committee should be reconvened in a matter of days to examine the situation further.
“Divergent views” is an understatement. There was firm opposition to the implementation of the PHEIC. 83 positive cases on January 30th “does not constitute a PHEIC”.
I should mention that the first PHEIC goes back to 2009. It was inaugurated by the WHO in relation to the H1N1 swine flu pandemic, which turned out to be a fraud.
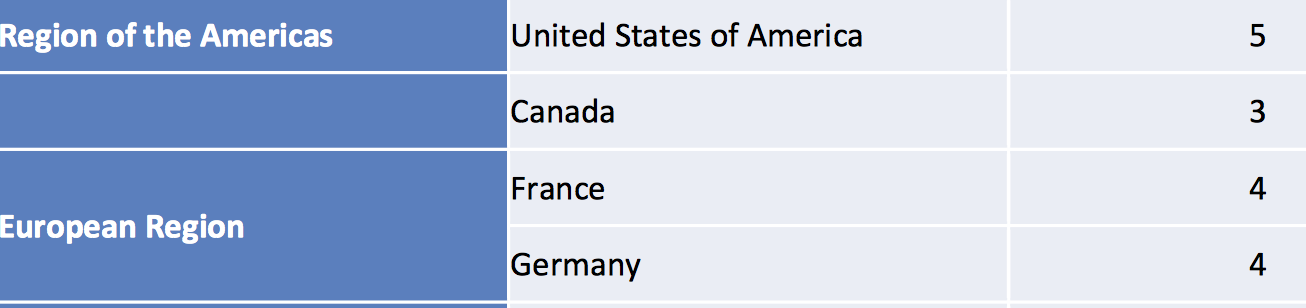
On January 29, 2020, the day preceding the launching of the PHEIC (recorded by the WHO), there were 5 cases in the US, 3 in Canada, 4 in France, 4 in Germany.
There was no “scientific basis” to justify the launching of a Worldwide public health emergency.
And bear in mind that the figures quoted above are based on Covid positive estimates generated by the contentious and disputed PCR-RT methodology
Screenshot of WHO table, January 29, 2020, (pdf document no longer available)
January 31, 2020: President Trump’s Decision to Suspend Air Travel with China
And these these ridiculously low numbers of Covid positive cases were then used by President Trump to suspend air travel to China on the following day (January 31, 2020).… Trump announced that he would deny entry to the US of both Chinese and foreign nationals “who have traveled in China in the last 14 days”. This immediately triggered a crisis in air travel, transportation, US-China trade relations as well as freight and shipping transactions.
…The five so-called “confirmed cases” in the US were sufficient to “justify” President Trump’s January 31st 2020 decision to suspend air travel to China while precipitating a hate campaign against ethnic Chinese throughout the Western World. (Michel Chossudovsky, E-Book Chapter II)
This historic January 31st 2020 decision paved the way towards the disruption of international commodity trade as well as the imposition of Worldwide restrictions on air travel. It has also led to the bankruptcy of major airlines, hotel chains and the tourist industry Worldwide.
And all they needed was 83 Covid Positive cases.
The next step of the COVID-19 saga unfolds on February 20, 2020.
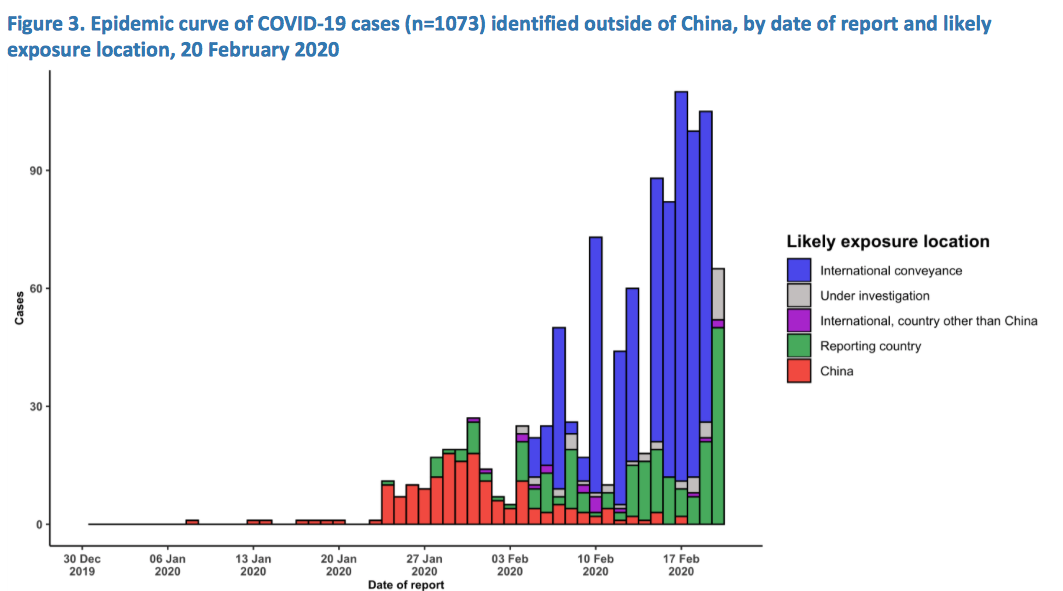
February 20-21, 2020. Dr. Tedros Intimates that the Pandemic is Imminent. 1073 Covid Positive Cases Outside China
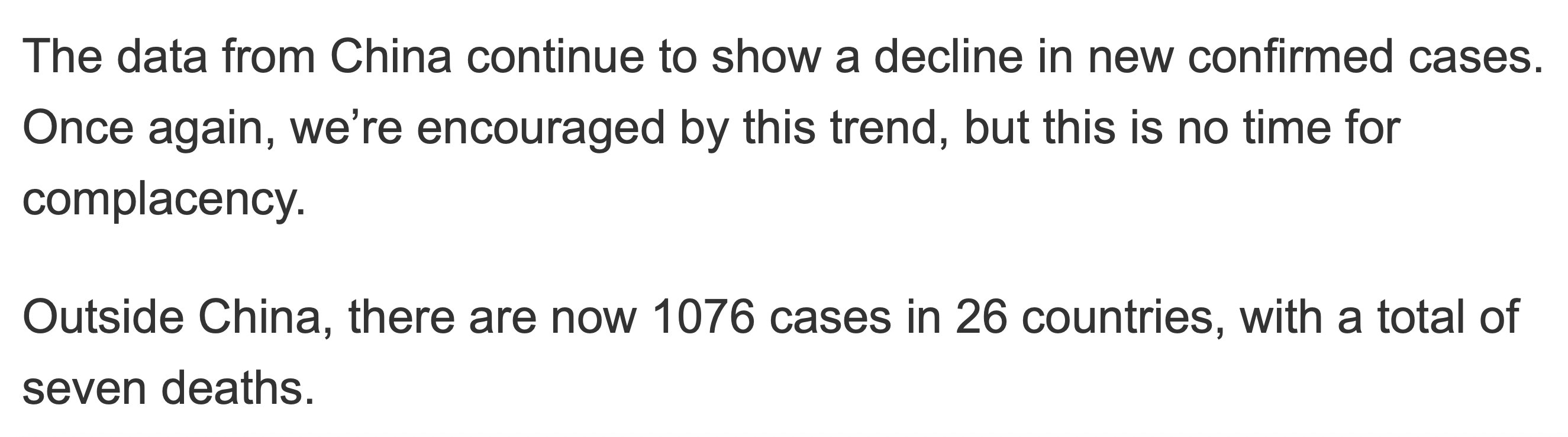
At a press conference on Thursday the 20th of February afternoon (CET Time) in a briefing in Geneva, the WHO Director General. Dr Tedros Adhanom Ghebreyesus, said that he was“concerned that the chance to contain the coronavirus outbreak was “closing” …
“I believe the window of opportunity is still there, but that the window is narrowing.”
Nonsense and outright lies. O

On that same day, 57.9 % of the Worldwide Covid-19 “confirmed cases” were from the Diamond Princess, hardly representative of a Worldwide “statistical trend”. From a statistical point of view, the WHO decision pointing to a potential “spread of the virus Worldwide” did not make sense.
A quarantine had been imposed on the cruiser See NCBI study. Many passengers fell sick due to the confinement on the boat. All the passengers and crew on the Diamond Princess undertook the PCR test. Without the Diamond Princess data, the so-called confirmed cases worldwide outside China on February 20th 2020 were of the order of 452, out of a population of 6.4 billion. (See the graph below indicating International Convenience (Diamond Princess))
Needless to say, this so-called data was instrumental to spearheading the fear campaign and the collapse of financial markets in the course of the month of February 2020.

Screenshot, WHO Press Conference, February 20th, 2020
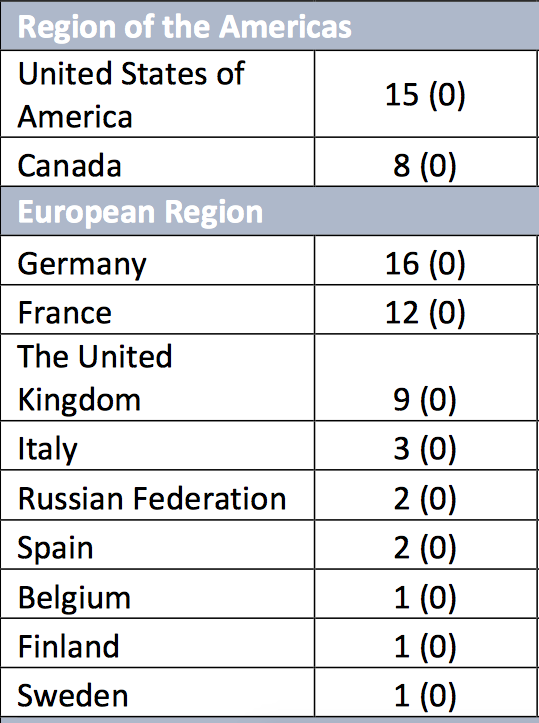
Note: The tabulated data above for February 20, 2020 indicates 1073 cases. 1076 cases in WHO Press Conference)
Dr. Tedros’ Statement (based on flawed concepts and statistics) had set the stage for the February 20-21 stock market collapse.
These are the figures (table right) used to support Tedros’ warnings that the pandemic is imminent.
Early March 2020
The recorded covid positive cases remain exceedingly low. On March 5, the WHO Director General confirms that outside China there are 2055 cases reported in 33 countries. Around 80% of those cases were from three countries (South Korea, Iran, Italy).On March 8, three days before the official launching of the Covid-19 Pandemic, the number of “confirmed cases” (infected and recovered) in the United States was of the order of 430, rising to about 600 on March 8, 2020.
Compare these ridiculously low figures to those pertaining to Influenza B Virus: The CDC estimated for 2019-2020 “at least 15 million [U.S] virus flu illnesses… 140,000 hospitalizations and 8,200 deaths. (The Hill)
It is worth noting that in early March, reported new cases in China fall to double digit. 99 cases recorded on March 7. All of the new cases outside Hubei province were categorized as “imported infections” (from foreign countries). The reliability of the data remains to be established:
While the outbreak in Hubei province was virtually over, the fake pandemic outside China launched on March 11, was commencing.99 newly confirmed cases including 74 in Hubei Province, … The new cases included 24 imported infections — 17 in Gansu Province, three in Beijing, three in Shanghai and one in Guangdong Province.
March 11, 2020: The Historic Covid-19 Pandemic, 44,279 “Confirmed Cases”
The WHO officially declared a Worldwide pandemic at a time when there were 44,279 confirmed cases outside China (6.4 billion population). Here is the justification of the WHO Director General regarding the WHO’s decision to declare a Worldwide pandemic:As I said on Monday, just looking at the number of cases and the number of countries affected does not tell the full story.
Of the 118,000 cases reported globally in 114 countries, more than 90 percent of cases are in just four countries, and two of those – China and the Republic of Korea – have significantly declining epidemics.
81 countries have not reported any cases, and 57 countries have reported 10 cases or less.

Nonsensical and contradictory statement. No evidence of an unfolding pandemic.
These are the figures used to justify the lockdown and the closing down of 190 national economies, with a view to saving lives.
In the US, recorded on March 11, 2020, there were according to John Hopkins: 1,335 “cases” and 29 deaths (“presumptive” plus PCR confirmed).
No evidence of a pandemic on March 11, 2020.
Immediately following the March 11, 2020 WHO announcement, the fear campaign went into high gear. Stock markets collapsed on the following day: Black Thursday.
On March 18, 2020 a lockdown was launched in the US.
The Upward Trend of Covid Positives In the Wake of the March 11, 2020 Lockdown
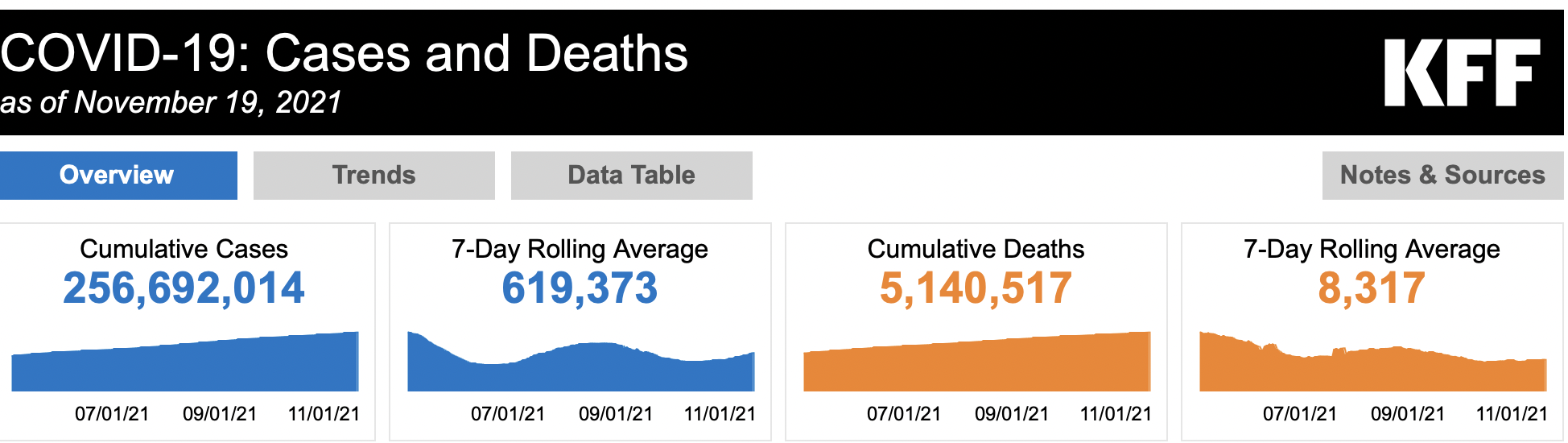
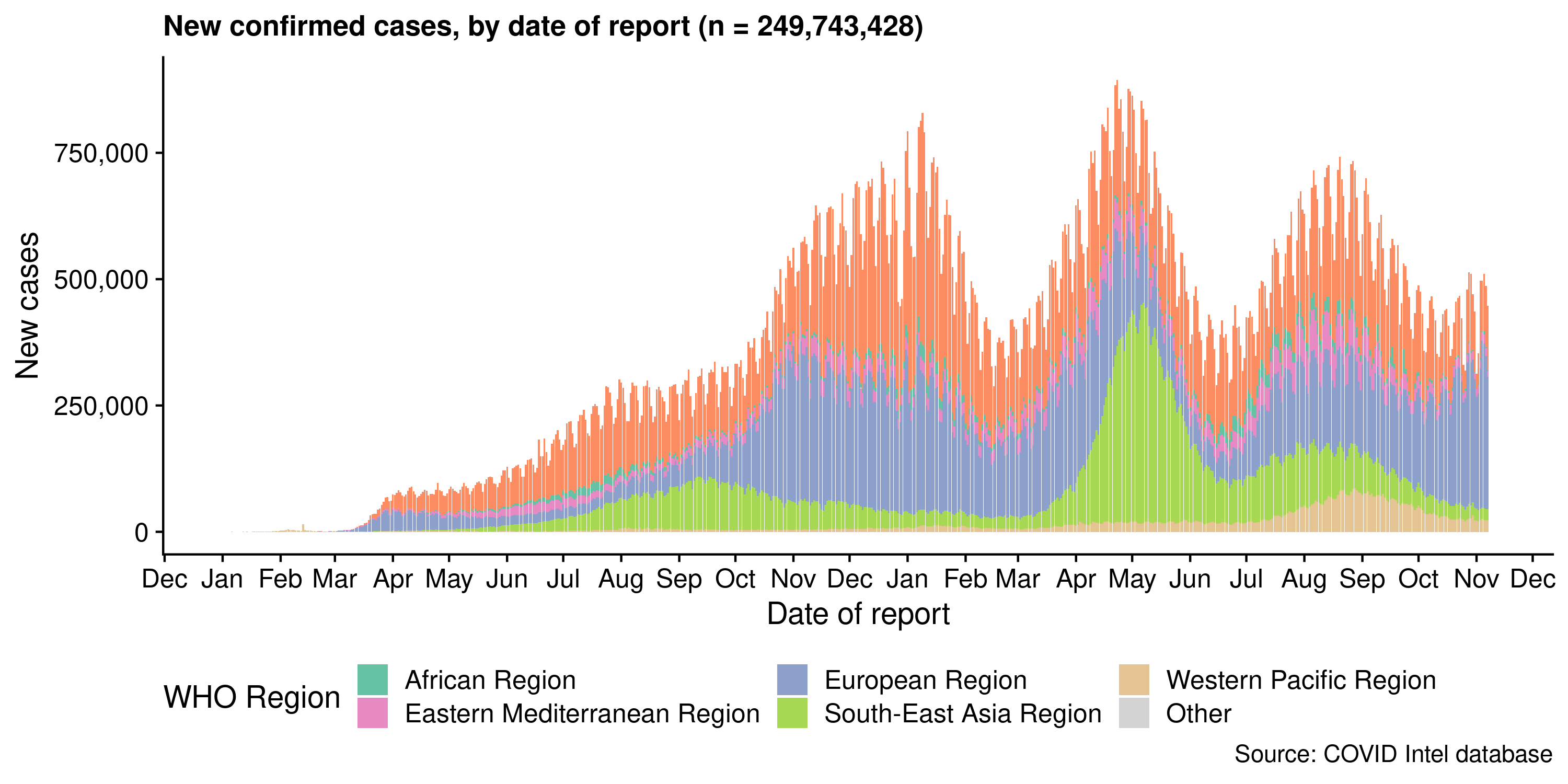
What can be observed in the diagram below is that the recorded Covid positive cases were exceedingly low prior to the official declaration of a pandemic on March 11, 2020: 44,279 cases outside China. There was absolutely no justification to launching the lockdown as a means to combating a non-existent “pandemic”.As of March 11, 2020, following the lockdown, national governments were urged to implement the PCR-RT test on a massive scale, with a view to pushing up the numbers of covid positive cases Worldwide.
Test, Test, Test: The numbers started to climb with a view to generating more and more fake statistics.
Look at the table below. A very small number of positive cases in early March. And then, Covid positive cases going fly high as of April, May June 2020.
***
In Part II, we will examine the role of the flawed PCR-RT Test and how it has been applied to sustaining the illusion of a Worldwide pandemic.
See Michel Chossudovsky’s E-Book, 13 Chapters:
The 2020-21 Worldwide Corona Crisis: Destroying Civil Society, Engineered Economic Depression, Global Coup d’État and the “Great Reset”
***
About the Author
Michel Chossudovsky is an award-winning author, Professor of Economics (emeritus) at the University of Ottawa, Founder and Director of the Centre for Research on Globalization (CRG), Montreal, Editor of Global Research.
He has undertaken field research in Latin America, Asia, the Middle East, sub-Saharan Africa and the Pacific and has written extensively on the economies of developing countries with a focus on poverty and social inequality. He has also undertaken research in Health Economics (UN Economic Commission for Latin America and the Caribbean (ECLAC), UNFPA, CIDA, WHO, Government of Venezuela, John Hopkins International Journal of Health Services (1979, 1983)
He is the author of twelve books including The Globalization of Poverty and The New World Order (2003), America’s “War on Terrorism” (2005), The Globalization of War, America’s Long War against Humanity (2015).
He is a contributor to the Encyclopaedia Britannica. His writings have been published in more than twenty languages. In 2014, he was awarded the Gold Medal for Merit of the Republic of Serbia for his writings on NATO’s war of aggression against Yugoslavia. He can be reached at [email protected]
See Michel Chossudovsky, Biographical Note
Michel Chossudovsky’s Articles on Global Research