news-medical.net
Is the BCG vaccine really protective against COVID-19?
By Dr. Liji Thomas, MDApr 26 2020
7-8 minutes
A new paper published on the preprint server medRxiv in April 2020 challenges the hypothesis that BCG vaccination confers some degree of protection against the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), which causes the pneumonic illness COVID-19.
The COVID-19 pandemic is still actively spreading across communities all over the world, in over 210 countries and territories. The total number of infections has crossed 2.9 million, with almost 206,000 deaths so far. The most significant case fatalities have been in the USA, Spain, Italy, France, and the UK, but the rates are increasing in many parts of the world.

Heterogeneous spread
Even though the pandemic began in China, its spread has been significantly uneven. After affecting a few Asian countries, mainly South Korea and Japan, it skipped continents to plague Europe and North America over the next six weeks. The rates at which infections have grown in various parts of the world are also quite different.
Researchers have been making desperate efforts to understand how the virus spreads and causes illness. A diverse spectrum of disease models has also emerged to attempt to predict the future burden of disease and the healthcare systems that will be necessary to care for the affected. However, the heterogeneous nature of the spread of COVID-19 is still largely unexplained, though several studies have evoked climatic differences to account for the perceived variations in the incidence, spread, and mortality rate of the disease.
Could the BCG vaccine play a role?
One such stream of research concerns the possible preventive role of the BCG (Bacille Calmette Guérin) vaccine. Since this vaccine is administered at widely different rates in different continents, and because its mechanism of action may involve non-specific boosting of immunity, some scientists postulated that it could have imparted greater immunity against the SARS-CoV-2 virus in countries where it is widely used.
The present study aims to examine the impact of BCG vaccination on the incidence and mortality of COVID-19 using the most recent data and after controlling for the number of tests per million population, or the effect of testing on the number of cases per million or deaths per million population. This is a vital omission since these variables depend on testing for detection.
How does testing affect case prevalence rates?
When the frequency of testing is very different between countries with similar infection rates or prevalence, and similar mortality rates, the result will be that they show a widely disparate number of cases and deaths per million. This is not because of a truly low prevalence or incidence or mortality, but because of the low testing rate in one country resulting in a low case detection rate.
It is known that low-income countries like Afghanistan have an abysmal testing rate of 13 per million population, while Iceland has over 100,000 tests per million (April 10, 2020, data). It is also clear that the number of cases and deaths per million is typically higher in those countries that are testing at much higher rates.
Analyzing the BCG effect
The current study seeks to extend research in this area in several ways. For one, the researchers use a new variable called the BCG Index rather than BCG itself. This is the proportion of a population that has received the BCG vaccine.
Secondly, they used additional controls to adjust for potential confounders such as the HDI scores, the period since the country had 1 case per million, the population density, the above-65 segment as a percentage of the population, the percentage of the population in urban areas and the Corruption Perception Index (CPI) that reflects the transparency of the government.
The third difference was in using tests per million and cases per test as dependent variables.
Finally, they verified the findings from the analysis of earlier studies using the most recent data
The researchers created multiple regression models, controlled for confounding demographic and economic factors, and for the period of reported spread. For instance, the time elapsed since a country reported its first 100 confirmed cases.
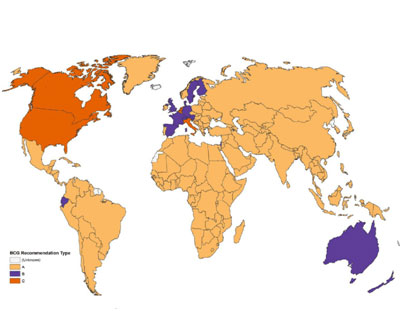
The BCG variable was in 3 tiers, comprising those who have never had scheduled BCG vaccination, those who have had it in the past but currently don’t have it. Those whose immunization schedules currently include it. The BCG Index is also included in the analysis, namely, the number of years since the BCG was made part of the immunization schedule in a country. The Index was created to improve the reliability of the data on BCG coverage in a population compared to a cross-sectional or snapshot study of the BCG inclusion in the immunization program.
The researchers then analyzed how the vaccine changed the rates of infection and death due to COVID-19 in that country, and particularly in how this effect endures when testing is controlled for, that is, by considering the number of tests per million population. They also looked at the cases per test (total number of cases per million divided by the number of tests per million).
What did the study show?
Like earlier studies, this time around too, the researchers found a link between the presence of routine BCG vaccination and fewer cases as well as deaths per million.
However, when the number of tests per million is accounted for, there is no longer any effect of BCG vaccination in reducing either the number of cases or deaths per million. Thus, factors like testing may have an impact on the routine administration of BCG and the caseload or mortality rate due to COVID-19 in a country.
Why is the study important?
The false security engendered by the impression that BCG coverage protects a population against COVID-19 could lead to poor policy decisions and bad judgment on the part of policymakers and healthcare workers alike. Universal BCG coverage is most likely in low-income countries, and these are the countries where reducing efforts to deal with COVID-19 by scaling up testing and recommending social distancing could be disastrous.
The researchers are currently setting up a dataset that will help measure the impact of the BCG vaccine over time rather than as a single snapshot.
Is the BCG vaccine really protective against COVID-19?
By Dr. Liji Thomas, MDApr 26 2020
7-8 minutes
A new paper published on the preprint server medRxiv in April 2020 challenges the hypothesis that BCG vaccination confers some degree of protection against the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), which causes the pneumonic illness COVID-19.
The COVID-19 pandemic is still actively spreading across communities all over the world, in over 210 countries and territories. The total number of infections has crossed 2.9 million, with almost 206,000 deaths so far. The most significant case fatalities have been in the USA, Spain, Italy, France, and the UK, but the rates are increasing in many parts of the world.
Heterogeneous spread
Even though the pandemic began in China, its spread has been significantly uneven. After affecting a few Asian countries, mainly South Korea and Japan, it skipped continents to plague Europe and North America over the next six weeks. The rates at which infections have grown in various parts of the world are also quite different.
Researchers have been making desperate efforts to understand how the virus spreads and causes illness. A diverse spectrum of disease models has also emerged to attempt to predict the future burden of disease and the healthcare systems that will be necessary to care for the affected. However, the heterogeneous nature of the spread of COVID-19 is still largely unexplained, though several studies have evoked climatic differences to account for the perceived variations in the incidence, spread, and mortality rate of the disease.
Could the BCG vaccine play a role?
One such stream of research concerns the possible preventive role of the BCG (Bacille Calmette Guérin) vaccine. Since this vaccine is administered at widely different rates in different continents, and because its mechanism of action may involve non-specific boosting of immunity, some scientists postulated that it could have imparted greater immunity against the SARS-CoV-2 virus in countries where it is widely used.
The present study aims to examine the impact of BCG vaccination on the incidence and mortality of COVID-19 using the most recent data and after controlling for the number of tests per million population, or the effect of testing on the number of cases per million or deaths per million population. This is a vital omission since these variables depend on testing for detection.
How does testing affect case prevalence rates?
When the frequency of testing is very different between countries with similar infection rates or prevalence, and similar mortality rates, the result will be that they show a widely disparate number of cases and deaths per million. This is not because of a truly low prevalence or incidence or mortality, but because of the low testing rate in one country resulting in a low case detection rate.
It is known that low-income countries like Afghanistan have an abysmal testing rate of 13 per million population, while Iceland has over 100,000 tests per million (April 10, 2020, data). It is also clear that the number of cases and deaths per million is typically higher in those countries that are testing at much higher rates.
Analyzing the BCG effect
The current study seeks to extend research in this area in several ways. For one, the researchers use a new variable called the BCG Index rather than BCG itself. This is the proportion of a population that has received the BCG vaccine.
Secondly, they used additional controls to adjust for potential confounders such as the HDI scores, the period since the country had 1 case per million, the population density, the above-65 segment as a percentage of the population, the percentage of the population in urban areas and the Corruption Perception Index (CPI) that reflects the transparency of the government.
The third difference was in using tests per million and cases per test as dependent variables.
Finally, they verified the findings from the analysis of earlier studies using the most recent data
The researchers created multiple regression models, controlled for confounding demographic and economic factors, and for the period of reported spread. For instance, the time elapsed since a country reported its first 100 confirmed cases.
The BCG variable was in 3 tiers, comprising those who have never had scheduled BCG vaccination, those who have had it in the past but currently don’t have it. Those whose immunization schedules currently include it. The BCG Index is also included in the analysis, namely, the number of years since the BCG was made part of the immunization schedule in a country. The Index was created to improve the reliability of the data on BCG coverage in a population compared to a cross-sectional or snapshot study of the BCG inclusion in the immunization program.
The researchers then analyzed how the vaccine changed the rates of infection and death due to COVID-19 in that country, and particularly in how this effect endures when testing is controlled for, that is, by considering the number of tests per million population. They also looked at the cases per test (total number of cases per million divided by the number of tests per million).
What did the study show?
Like earlier studies, this time around too, the researchers found a link between the presence of routine BCG vaccination and fewer cases as well as deaths per million.
However, when the number of tests per million is accounted for, there is no longer any effect of BCG vaccination in reducing either the number of cases or deaths per million. Thus, factors like testing may have an impact on the routine administration of BCG and the caseload or mortality rate due to COVID-19 in a country.
Why is the study important?
The false security engendered by the impression that BCG coverage protects a population against COVID-19 could lead to poor policy decisions and bad judgment on the part of policymakers and healthcare workers alike. Universal BCG coverage is most likely in low-income countries, and these are the countries where reducing efforts to deal with COVID-19 by scaling up testing and recommending social distancing could be disastrous.
The researchers are currently setting up a dataset that will help measure the impact of the BCG vaccine over time rather than as a single snapshot.