
- Joined
- Jul 10, 2008
- Messages
- 67,525
- Points
- 113
drjohnm.org
Can We Discuss Flatten-the-Curve in COVID19? My Eight Assertions
9-12 minutes
On Telehealth, an older couple asked me a tough question about COVID19. They asked whether this virus would either be gone or less dangerous in 6 months to a year.
It was a curious question. I replied, Why do you ask?
Indeed my patient was correct. Dr. Scott Gottlieb writing in the WSJ, did not mince words:
In essence, my couple asks whether flatten-the-curve policies save lives. Buried in that question are three other questions: namely, in one year, will the virus be 1) gone, or 2) less contagious, or 3) less deadly? If any of those three are true, then my couple could rationally decide to stay lonely for a year or more.
I study this new virus and this once-in-a-lifetime-situation every day.
I don’t think flatten-the-curve policies will change any of those issues. Let me explain my reasoning. I may be wrong; tell me if you disagree in the comments.
Flatten-the-Curve Purpose
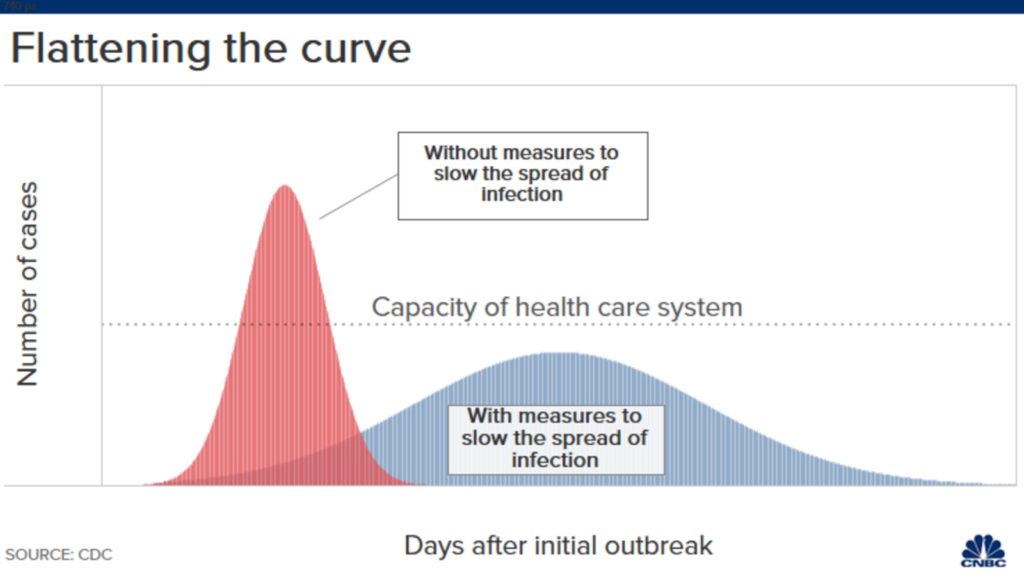
You now know the famous curves–one with an early surge of disease, and the other flatter curve that spreads the infections over time. The y-axis is number of COVID19 cases.
In early March the COVID19 narratives were from Wuhan, Iran, Lombardy and Spain, places where surges overwhelmed hospitals. In the US, COVID cases spiked in NYC.
Early COVID19 surges were over-running some big-city hospitals. This was bad because it caused excess or preventable death–people who could have been saved were not saved because of shortages of ICU beds, dialysis equipment, staff and ventilators.
Social distancing policies and postponement of elective medical care were necessary to stop the excess deaths. These policies allowed time for hospitals to prepare for COVID19 cases and for doctors to learn how best to treat these patients. Exhibit A: not intubating patients early.
Social distancing worked. The number of cases slowed and the US got into the blue part of the curve. But now, months later, the narrative has changed.
Change in Flatten-the-Curve Narrative
What was once flatten the curve to prevent over-running hospitals has changed to flatten the curve to save lives. Some likened moderation of social distancing to human sacrifice.
That change in framing, I believe, is misleading. I will argue that the cumulative deaths from COVID19 will not be reduced significantly by flatten-the-curve policies. And that this virus will be as dangerous to vulnerable patients in 6 months to a year. We should be allowed to debate this.
My case has eight assertions.
First: the virus will not be contained. The chance for containment has long passed. The virus transmits before people know they have it and many patients never develop symptoms. It will be with us until an effective vaccine is both widely available and widely used. (See #6)
Second: Tests will under-perform. The high rate of asymptomatic disease, the low sensitivity of PCR tests (false negatives), imperfect specificity of antibody tests (false positives) and concerns over privacy mean that we should expect less from test and trace–even if proposed by a Nobel Laureate. Carl Bergstrom and others write persuasively on major barriers to contact tracing in the US.
Third: US hospitals are now prepared and in little danger of being over-whelmed. In fact, many hospitals are so dormant they are nearing financial ruin. Healthcare workers have been furloughed due to postponement of elective work. I’ve talked to numerous colleagues in the US and the message is clear: hospitals are under-capacity and prepared for a “persistent” number of COVID19 cases during the coming months/years. Hospitals now have COVID response teams.
Fourth: Americans are not stupid. Before governors enacted lockdowns, economic activity and travel slowed, the NBA, MBL, NHL stopped their seasons and medical meetings were cancelled. People socially distance not because police are bearing down on them, but because it makes sense. The pictures of spring-breakers in Florida and crazies-with-guns in state capitals bring clicks to news organizations but belie the majority of sensible people in this country.
Fifth: Public-health surveillance has improved. Tests may underperform but they will not be useless. Tests will help signal coming hot spots and that will allow communities to act locally. Other technologies may emerge that help prevent surges. One cool example is the use of resting heart rate apps that might signal health officials early on.
Sixth: (I need a few paragraphs): Social distancing will not lower the infection fatality rate or IFR. Remember the red and blue curves? The y-axis of that graph is number of infections. Due to the contagion of this virus, the area under these curves is likely to be the same at the end of two years. Ok, then, if the number of cases is similar at two years, then the number of people who cumulatively die will not likely change either.
The only way fewer people die from COVID19 over time is if the IFR declines. Here is where American exceptionalism misleads people. Politicians have a strong bias to pump up optimism on any potential medical advance–no matter how dubious. (Exhibit B- hydroxychloroquine.)
That is not how Medicine works. History is replete with examples showing that drug development is super hard. But leaving aside the challenge of developing new drugs against a new virus, the basic math of COVID19 creates a huge barrier for success: already, more than 99% of people infected with this virus survive. A therapy that has a massive 50% reduction in death from a disease with 1% mortality (high estimate) delivers only a 0.5% absolute risk reduction.
What about Remdesivir? This antiviral may help a little. But even if you believe its ≈ 3% reduction of death was not due to chance (p = 0.06), the death rate in the remdesivir arm in that trial was 8%. Remdesivir is no game-changer.
COVID19 vaccine development is sobering. Most experts say a safe and effective vaccine is at least 18 months away. Again, the 99% survivability erects a huge safety barrier for vaccine makers. (I get that from Dr. Paul Offit.) Given society’s tension over vaccines, it would take only a tiny signal of harm to derail a coronavirus vaccine.
A slight hedge on the sixth assertion that IFR remains constant: some smart people say that getting the virus later may be better because doctors will be a little better at treating this disease. For instance, a year from now we may better understand how to use drugs that block clotting; we may have better vent protocols. These are big ifs. They may drive the IFR down a little but IFR is already low. Another benefit of infection in a year would be that most hospitals will likely allow family visitors.
Seventh: The more we test, the lower the IFR goes. Early estimates had it at 3%. Then it was revised downward to about 1%. Now most people put it at 0.1-0.5%. But that is still quite serious. You’ve probably read that 0.1% is similar to flu mortality. That is likely wrong. Dr. Jeremy Faust points out that flu mortality is grossly overestimated and is probably much lower than 0.1%.
Eighth: I wrote a piece on Medscape about the harms from COVID19 interventions. One of the points I made is that right now we count only deaths from COVID19. We stay riveted on day-to-day numbers. But the endpoint of this crisis is not next month but in 1-2 years. And when we get there, we have to count people who died from COVID19 and those who died from other causes.
This preprint from prominent researchers suggests a substantial proportion of excess deaths observed during the pandemic are not attributed to COVID19 and may represent an excess of deaths due to other causes.
In my column I cited an older study by Raj Chetty and co-workers that finds a strong association of lower income and lower survival. And that is the rub with COVID19 interventions: they make poor people even poorer. The rich just work from home. It is possible, therefore, that our social interventions will be especially hard on the disadvantaged.
I realize that no person overtly dismisses the harm from economic shutdowns. My friend Dr. Dan Morgan expresses my frustrations well in this thread. Why can one safely critique a drug for COVID19 but not massive public health interventions?
Conclusion:
I did not have a clear answer for my couple. But after thinking and writing about this question it seems that the most reasonable approach in this crisis is transparent information–no matter how stark. And, crucially, we must have space for public debate.
I hate this virus. I wish it never came. But we can make it worse by avoiding hard discussions on tradeoffs, the limits of modern medicine and risk.
JMM
P.S. I am very interested in your rebuttals to any of my assertions but will block vitriol and politicized nonsense.
Can We Discuss Flatten-the-Curve in COVID19? My Eight Assertions
9-12 minutes
On Telehealth, an older couple asked me a tough question about COVID19. They asked whether this virus would either be gone or less dangerous in 6 months to a year.
It was a curious question. I replied, Why do you ask?
Doc, we have a big family with many children and grandchildren, most of whom live nearby. We miss them. We’ve been isolating, but it’s hard; we did it for 6 weeks. Doing it for a year or more would be miserable.
We saw on the news today that the battle with the virus would be long. A man called it a cruel new normal.
So doc, if you tell me the the virus will be gone in a year or it will be less dangerous to get infected later, then it makes sense for us to keep isolating. But if the situation will not be much different a year from now, we would just as soon see our family and take the risk. Of course, doc, we would still be sensible. We’d not visit if someone was sick; we would wash our hands and wear masks.
Indeed my patient was correct. Dr. Scott Gottlieb writing in the WSJ, did not mince words:
Hospitals and public-health systems will have to contend with persistent disease and death.
In essence, my couple asks whether flatten-the-curve policies save lives. Buried in that question are three other questions: namely, in one year, will the virus be 1) gone, or 2) less contagious, or 3) less deadly? If any of those three are true, then my couple could rationally decide to stay lonely for a year or more.
I study this new virus and this once-in-a-lifetime-situation every day.
I don’t think flatten-the-curve policies will change any of those issues. Let me explain my reasoning. I may be wrong; tell me if you disagree in the comments.
Flatten-the-Curve Purpose
You now know the famous curves–one with an early surge of disease, and the other flatter curve that spreads the infections over time. The y-axis is number of COVID19 cases.
In early March the COVID19 narratives were from Wuhan, Iran, Lombardy and Spain, places where surges overwhelmed hospitals. In the US, COVID cases spiked in NYC.
Early COVID19 surges were over-running some big-city hospitals. This was bad because it caused excess or preventable death–people who could have been saved were not saved because of shortages of ICU beds, dialysis equipment, staff and ventilators.
Social distancing policies and postponement of elective medical care were necessary to stop the excess deaths. These policies allowed time for hospitals to prepare for COVID19 cases and for doctors to learn how best to treat these patients. Exhibit A: not intubating patients early.
Social distancing worked. The number of cases slowed and the US got into the blue part of the curve. But now, months later, the narrative has changed.
Change in Flatten-the-Curve Narrative
What was once flatten the curve to prevent over-running hospitals has changed to flatten the curve to save lives. Some likened moderation of social distancing to human sacrifice.
That change in framing, I believe, is misleading. I will argue that the cumulative deaths from COVID19 will not be reduced significantly by flatten-the-curve policies. And that this virus will be as dangerous to vulnerable patients in 6 months to a year. We should be allowed to debate this.
My case has eight assertions.
First: the virus will not be contained. The chance for containment has long passed. The virus transmits before people know they have it and many patients never develop symptoms. It will be with us until an effective vaccine is both widely available and widely used. (See #6)
Second: Tests will under-perform. The high rate of asymptomatic disease, the low sensitivity of PCR tests (false negatives), imperfect specificity of antibody tests (false positives) and concerns over privacy mean that we should expect less from test and trace–even if proposed by a Nobel Laureate. Carl Bergstrom and others write persuasively on major barriers to contact tracing in the US.
Third: US hospitals are now prepared and in little danger of being over-whelmed. In fact, many hospitals are so dormant they are nearing financial ruin. Healthcare workers have been furloughed due to postponement of elective work. I’ve talked to numerous colleagues in the US and the message is clear: hospitals are under-capacity and prepared for a “persistent” number of COVID19 cases during the coming months/years. Hospitals now have COVID response teams.
Fourth: Americans are not stupid. Before governors enacted lockdowns, economic activity and travel slowed, the NBA, MBL, NHL stopped their seasons and medical meetings were cancelled. People socially distance not because police are bearing down on them, but because it makes sense. The pictures of spring-breakers in Florida and crazies-with-guns in state capitals bring clicks to news organizations but belie the majority of sensible people in this country.
Fifth: Public-health surveillance has improved. Tests may underperform but they will not be useless. Tests will help signal coming hot spots and that will allow communities to act locally. Other technologies may emerge that help prevent surges. One cool example is the use of resting heart rate apps that might signal health officials early on.
Sixth: (I need a few paragraphs): Social distancing will not lower the infection fatality rate or IFR. Remember the red and blue curves? The y-axis of that graph is number of infections. Due to the contagion of this virus, the area under these curves is likely to be the same at the end of two years. Ok, then, if the number of cases is similar at two years, then the number of people who cumulatively die will not likely change either.
The only way fewer people die from COVID19 over time is if the IFR declines. Here is where American exceptionalism misleads people. Politicians have a strong bias to pump up optimism on any potential medical advance–no matter how dubious. (Exhibit B- hydroxychloroquine.)
That is not how Medicine works. History is replete with examples showing that drug development is super hard. But leaving aside the challenge of developing new drugs against a new virus, the basic math of COVID19 creates a huge barrier for success: already, more than 99% of people infected with this virus survive. A therapy that has a massive 50% reduction in death from a disease with 1% mortality (high estimate) delivers only a 0.5% absolute risk reduction.
What about Remdesivir? This antiviral may help a little. But even if you believe its ≈ 3% reduction of death was not due to chance (p = 0.06), the death rate in the remdesivir arm in that trial was 8%. Remdesivir is no game-changer.
COVID19 vaccine development is sobering. Most experts say a safe and effective vaccine is at least 18 months away. Again, the 99% survivability erects a huge safety barrier for vaccine makers. (I get that from Dr. Paul Offit.) Given society’s tension over vaccines, it would take only a tiny signal of harm to derail a coronavirus vaccine.
A slight hedge on the sixth assertion that IFR remains constant: some smart people say that getting the virus later may be better because doctors will be a little better at treating this disease. For instance, a year from now we may better understand how to use drugs that block clotting; we may have better vent protocols. These are big ifs. They may drive the IFR down a little but IFR is already low. Another benefit of infection in a year would be that most hospitals will likely allow family visitors.
Seventh: The more we test, the lower the IFR goes. Early estimates had it at 3%. Then it was revised downward to about 1%. Now most people put it at 0.1-0.5%. But that is still quite serious. You’ve probably read that 0.1% is similar to flu mortality. That is likely wrong. Dr. Jeremy Faust points out that flu mortality is grossly overestimated and is probably much lower than 0.1%.
Eighth: I wrote a piece on Medscape about the harms from COVID19 interventions. One of the points I made is that right now we count only deaths from COVID19. We stay riveted on day-to-day numbers. But the endpoint of this crisis is not next month but in 1-2 years. And when we get there, we have to count people who died from COVID19 and those who died from other causes.
This preprint from prominent researchers suggests a substantial proportion of excess deaths observed during the pandemic are not attributed to COVID19 and may represent an excess of deaths due to other causes.
In my column I cited an older study by Raj Chetty and co-workers that finds a strong association of lower income and lower survival. And that is the rub with COVID19 interventions: they make poor people even poorer. The rich just work from home. It is possible, therefore, that our social interventions will be especially hard on the disadvantaged.
I realize that no person overtly dismisses the harm from economic shutdowns. My friend Dr. Dan Morgan expresses my frustrations well in this thread. Why can one safely critique a drug for COVID19 but not massive public health interventions?
Conclusion:
I did not have a clear answer for my couple. But after thinking and writing about this question it seems that the most reasonable approach in this crisis is transparent information–no matter how stark. And, crucially, we must have space for public debate.
I hate this virus. I wish it never came. But we can make it worse by avoiding hard discussions on tradeoffs, the limits of modern medicine and risk.
JMM
P.S. I am very interested in your rebuttals to any of my assertions but will block vitriol and politicized nonsense.
