
-
IP addresses are NOT logged in this forum so there's no point asking. Please note that this forum is full of homophobes, racists, lunatics, schizophrenics & absolute nut jobs with a smattering of geniuses, Chinese chauvinists, Moderate Muslims and last but not least a couple of "know-it-alls" constantly sprouting their dubious wisdom. If you believe that content generated by unsavory characters might cause you offense PLEASE LEAVE NOW! Sammyboy Admin and Staff are not responsible for your hurt feelings should you choose to read any of the content here. The OTHER forum is HERE so please stop asking.
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
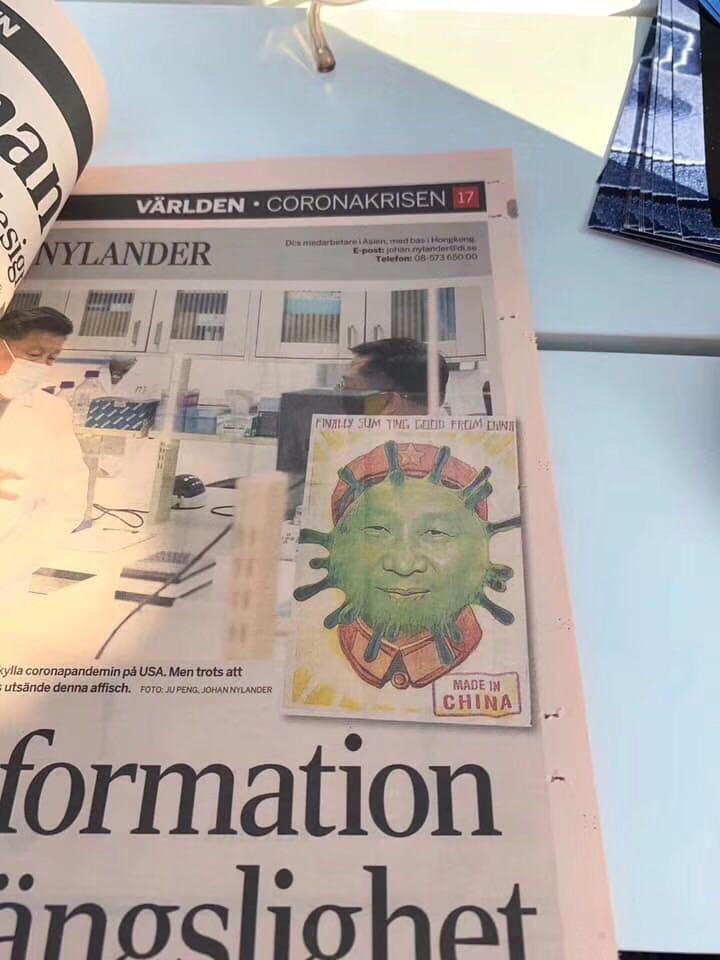
Swedes are given freedom to decide for themselves!
- Thread starter nayr69sg
- Start date
- Joined
- Jul 10, 2008
- Messages
- 67,737
- Points
- 113
Thankfully there are still some sanity left in this world.
In the article I still see medical professionals critical of the lack of action.
Would they voice the same opinion if 50% of their income came from their salaries as a doc and the other 50% came from owning a pub?
In the article I still see medical professionals critical of the lack of action.
Would they voice the same opinion if 50% of their income came from their salaries as a doc and the other 50% came from owning a pub?
Thankfully there are still some sanity left in this world.
In the article I still see medical professionals critical of the lack of action.
Would they voice the same opinion if 50% of their income came from their salaries as a doc and the other 50% came from owning a pub?
LOL!
Actually unless you are the Chief Medical Officer or some chief of Infectious Disease or Communicable disease , as a doctor you have ZERO influence lah.
ZERO. ZILCH.
The politicians wont listen to you. And if you speak out of line you risk having complaints against you from those very Chiefs and you think the College will side with you speaking outside of your specialty?
It is all POLITICAL. Be it in the actual political sphere or among doctors in inner politics.
So all these decisions are made based on the recommendations of a small handful of SPECIALISTS.
There has never been a vote or poll made to doctors in general about what they think should be done. Did they have some big townhall meeting to ask us? Nope.
It is just probably ONE doctor calling the shots.
Just got this email from the CPSA. Does it look to you like even the College knows what the hell is happening?
Like I said it is the Chief Medical Officer ordering this and that. And we just follow
CPSA Advice to the Profession: Defining "Urgent" During COVID-19
This is applicable for the duration of the COVID-19 pandemic
CPSA Perspective
Physicians should not be reluctant to provide care, even when it may be extremely difficult to follow some components of CPSA’s Standards of Practice. CPSA will always consider the individual circumstances and context if a complaint arises during the COVID-19 pandemic. In an emergency situation, failure to meet standards is not considered unprofessional conduct if a physician can demonstrate they took all reasonable actions in their service to patients.
What is the definition of “urgency”?
Due to the COVID-19 pandemic, physicians have been required to discontinue the provision of non-essential health services and limit practice to “services deemed urgent by the health professional providing the service” (CMOH Order 07-2020). As a result, CPSA has been asked for guidance on how we, as a profession, define what care is considered urgent.
There is no simple answer. What is urgent is dependent on many factors in each unique clinical context. Patients will continue to have medical problems which require assessment and therapy, and, at times, this may need to be in person. For example, some patients will still require surgeries during the pandemic. Weighing the benefit of providing care with preventing the spread of COVID-19 by delaying appointments and procedures will be a constant challenge.
CPSA has been asked for very clear and specific messaging on this, but this is not possible. As a self-regulating profession, our expectation is that physicians will collaborate with colleagues in similar practices when making these decisions. It’s important to share best evidence, get advice from guiding professional organizations and draw on your personal experience. This will help guide practice and decrease some of the pressure many physicians are feeling to ensure they are making the best choices possible under difficult circumstances.
Considerations in determining urgency
An important first step is to consider what work we should not be doing at this time. As per the recent Order by the Chief Medical Officer of Health, “a ‘non-essential health service’ includes any service that is generally done to protect, promote or maintain health of an individual and where an interruption in the provision of services will not result in an individual’s life, health or safety being immediately endangered” (CMOH Order 07-2020).
There are a few situations more obviously considered to be non-essential and, therefore, deferred, such as routine health monitoring and cosmetic procedures. Physicians should encourage Albertans to adhere to the Chief Medical Officer of Health’s advice to remain home unless absolutely essential. Using virtual care as a means to assess urgency can be informative in planning. Please review the COVID-19 Virtual Care Advice to the Profession.
Next, we need to decide what care we should be providing at this time. A few questions to consider when determining if care is urgent include:
Does the patient feel the benefit of therapy exceeds the risk of the leaving their home?
Is the benefit to the individual patient worth the risk of having them leave their home? Special consideration must be given to high-risk patients (e.g.: patients with pre-existing health conditions or who are over 60 years old)
Could scarce resources, like acute care, need to be accessed if the procedure does not go as planned? How will this be coordinated?
Will the care provided prevent the need for a patient to access acute care in the foreseeable future?
Would a group of peers support the decision the care is urgent? Would colleagues perceive these actions as being self-serving, rather than putting the needs of patients, staff and society first?
Urgency is complex – there is no one single answer. As a self-regulating profession, physicians must work closely together to determine what is best for their patients and recognize the need to be flexible in our thinking as we adjust to the evolving situation. We trust physicians will make decisions in the best interest of the public good.
Adhering to Public Health orders
CPSA has received concerns from Albertans, public health and other physicians about some physicians not following the recommendations from the Chief Medical Officer of Health and continuing business as usual. We will address these concerns by reaching out to individual physicians to support navigating this decision making.
To date, most concerns have been addressed effectively in this manner. In the unusual circumstance a physician chooses to ignore this direction and continues to put the public at risk, we will address these situations in more formal ways through our complaints process and referral to the local Medical Officer of Health.
Resources
In addition to this guidance on medical services provision, please follow Alberta Health’s public health orders on self-isolation and recommendations on preventing spread. Additional resources are available in AHS’ COVID-19 information for primary care providers (infection prevention & control, PPE, testing, etc.) and CPSA resources for physicians during COVID-19 (virtual health care, COVID-19 physician registry, etc.).
Like I said it is the Chief Medical Officer ordering this and that. And we just follow
CPSA Advice to the Profession: Defining "Urgent" During COVID-19
This is applicable for the duration of the COVID-19 pandemic
CPSA Perspective
Physicians should not be reluctant to provide care, even when it may be extremely difficult to follow some components of CPSA’s Standards of Practice. CPSA will always consider the individual circumstances and context if a complaint arises during the COVID-19 pandemic. In an emergency situation, failure to meet standards is not considered unprofessional conduct if a physician can demonstrate they took all reasonable actions in their service to patients.
What is the definition of “urgency”?
Due to the COVID-19 pandemic, physicians have been required to discontinue the provision of non-essential health services and limit practice to “services deemed urgent by the health professional providing the service” (CMOH Order 07-2020). As a result, CPSA has been asked for guidance on how we, as a profession, define what care is considered urgent.
There is no simple answer. What is urgent is dependent on many factors in each unique clinical context. Patients will continue to have medical problems which require assessment and therapy, and, at times, this may need to be in person. For example, some patients will still require surgeries during the pandemic. Weighing the benefit of providing care with preventing the spread of COVID-19 by delaying appointments and procedures will be a constant challenge.
CPSA has been asked for very clear and specific messaging on this, but this is not possible. As a self-regulating profession, our expectation is that physicians will collaborate with colleagues in similar practices when making these decisions. It’s important to share best evidence, get advice from guiding professional organizations and draw on your personal experience. This will help guide practice and decrease some of the pressure many physicians are feeling to ensure they are making the best choices possible under difficult circumstances.
Considerations in determining urgency
An important first step is to consider what work we should not be doing at this time. As per the recent Order by the Chief Medical Officer of Health, “a ‘non-essential health service’ includes any service that is generally done to protect, promote or maintain health of an individual and where an interruption in the provision of services will not result in an individual’s life, health or safety being immediately endangered” (CMOH Order 07-2020).
There are a few situations more obviously considered to be non-essential and, therefore, deferred, such as routine health monitoring and cosmetic procedures. Physicians should encourage Albertans to adhere to the Chief Medical Officer of Health’s advice to remain home unless absolutely essential. Using virtual care as a means to assess urgency can be informative in planning. Please review the COVID-19 Virtual Care Advice to the Profession.
Next, we need to decide what care we should be providing at this time. A few questions to consider when determining if care is urgent include:
Does the patient feel the benefit of therapy exceeds the risk of the leaving their home?
Is the benefit to the individual patient worth the risk of having them leave their home? Special consideration must be given to high-risk patients (e.g.: patients with pre-existing health conditions or who are over 60 years old)
Could scarce resources, like acute care, need to be accessed if the procedure does not go as planned? How will this be coordinated?
Will the care provided prevent the need for a patient to access acute care in the foreseeable future?
Would a group of peers support the decision the care is urgent? Would colleagues perceive these actions as being self-serving, rather than putting the needs of patients, staff and society first?
Urgency is complex – there is no one single answer. As a self-regulating profession, physicians must work closely together to determine what is best for their patients and recognize the need to be flexible in our thinking as we adjust to the evolving situation. We trust physicians will make decisions in the best interest of the public good.
Adhering to Public Health orders
CPSA has received concerns from Albertans, public health and other physicians about some physicians not following the recommendations from the Chief Medical Officer of Health and continuing business as usual. We will address these concerns by reaching out to individual physicians to support navigating this decision making.
To date, most concerns have been addressed effectively in this manner. In the unusual circumstance a physician chooses to ignore this direction and continues to put the public at risk, we will address these situations in more formal ways through our complaints process and referral to the local Medical Officer of Health.
Resources
In addition to this guidance on medical services provision, please follow Alberta Health’s public health orders on self-isolation and recommendations on preventing spread. Additional resources are available in AHS’ COVID-19 information for primary care providers (infection prevention & control, PPE, testing, etc.) and CPSA resources for physicians during COVID-19 (virtual health care, COVID-19 physician registry, etc.).
- Joined
- Oct 7, 2012
- Messages
- 5,228
- Points
- 113
All the clowns complaining about unnecessary lockdowns are actually so called “long term investors” who lost money betting on a V shaped stock market recovery based on half baked guesses that this thing will be similar to SARS. This should teach them a lesson to make superficial extrapolations from the past, but it won’t, because most humans are stubborn and only want to hear what they want to hear, including so called “doc” aka pharmacy dispenser who gives his patients what they want. LOL.
All the clowns complaining about unnecessary lockdowns are actually so called “long term investors” who lost money betting on a V shaped stock market recovery based on half baked guesses that this thing will be similar to SARS. This should teach them a lesson to make superficial extrapolations from the past, but it won’t, because most humans are stubborn and only want to hear what they want to hear, including so called “doc” aka pharmacy dispenser who gives his patients what they want. LOL.
hey what did I do to you that you have to attack me personally?
- Joined
- Oct 7, 2012
- Messages
- 5,228
- Points
- 113
hey what did I do to you that you have to attack me personally?
being your usual kaypohchee self

being your usual kaypohchee self
ok ok. I think I know what triggered you.
Apologies. I will make a note not to mention that about you again.
Hey take it easy ok bro? Chill man.
All the clowns complaining about unnecessary lockdowns are actually so called “long term investors” who lost money betting on a V shaped stock market recovery based on half baked guesses that this thing will be similar to SARS. This should teach them a lesson to make superficial extrapolations from the past, but it won’t, because most humans are stubborn and only want to hear what they want to hear, including so called “doc” aka pharmacy dispenser who gives his patients what they want. LOL.
Actually only way to confirm a losing "trade" is when you complete a buy and sell. Or if you bought a company that went bankrupt or was sold and went private.
So I have lost NO MONEY WHATSOEVER so far. In fact I have realized some profit from closing my position on Transcanada Pipelines.
Traders have the disadvantage of having to close their positions in a short term especially with short positions because they losses can be infinite as long as the stock keeps going up!!!!! Whereas with long positions the losses are capped based on what you bet.
I am sure there are more sophisticated instruments out there and I am talking through my arse when seasoned veteran traders read my rubbish. But it is true that you can only realize any loss when you close the positions you have. Same with long trades except for some companies they do pay you dividend.
It is very different if you want to trade vs invest in companies.
Trading you need a lot of discipline and nerves of steel, be able to take the lows and highs in emotions. This is not my cup of tea.
- Joined
- Oct 7, 2012
- Messages
- 5,228
- Points
- 113
ok ok. I think I know what triggered you.
Apologies. I will make a note not to mention that about you again.
Hey take it easy ok bro? Chill man.
U have all the kaypohchee and fake characteristics and behaviour of that moron screwed ball. Whether I are same or different person is besides the point. Go back to your dream of being a cannabis dispensing automaton.

U have all the kaypohchee and fake characteristics and behaviour of that moron screwed ball. Whether I are same or different person is besides the point. Go back to your dream of being a cannabis dispensing automaton.
Eh don't insult lah. I am not a cannabis dispensing automaton.
I dispense nothing
I only write prescriptions. How many grams/day. And the grams/day is not really how much the patient uses. It is an authorization to how much they can buy.
The Federal Law for ACMPR when it started was to allow patients to be able to legally possess cannabis for medical purposes. Back then mostly people all carry dried flower or milled cannabis. So if they had 2g/day prescription, then it means they can at any time possess 30 day supply ie 60g. Police will weigh and see if below 60g.
These days medical patients use mostly oils. and every Licenced Producer (LP) has a conversion factor.
https://hmed.ca/oil-equivalency-jun-2019/
Eg most LPs would be able to produce 5-8 ml of CBD or THC oil from 1g of dried cannabis. When I explain to my patients I usually use the 1g = 8ml of oil So a 40ml bottle used 5g of dried cannabis to make. Hence if you have a prescription of 1g/day then you are allowed to buy 6 bottles of oil per month or a mix of oil and actual weight of dried flower.
Often we increase the prescription amount not because they actually use that much but because patients want to have more than one LP. Eg they might want to go with Spectrum Cannabis, Aurora Cannabis and Cannimed. Then we write 3g/day and send 1g/day to each of the 3 LPs.
Shoppers Drug Mart is an LP but they dont grow their own cannabis. Through their portal you have access to 12 differnt LPs. You dont get access to all the products in each LP under the SDM umbrella but at least you get more variety.
So there are various nuances in the medical cannabis market.
Patients dont get their prescriptions. We send it to the LPs they want to sign up with. The patient will go on the website and register. Then the LP sends a confirmation email back to them indicating they can order product. They put in orders online or over the phone pay using credit card and then the products are mailed to their address on file.
CPSA requires all physicians writing medical cannabis authorizations to see their patients for follow ups at minimum intervals of 3 months. This is the standard of practice. So every patient has to see the doctor at least 4 times a year.
Since legalization the number of patients wanting prescriptions has dropped considerably since you can just walk to the recreational store and get THC CBD and what not.
Hence the practice of medical cannabis now is very much made up of genuine patients who require help with anxiety, insomnia, chronic pain (top 3 conditions). We do get the GI patients eg IBS IBD, Celiac, migraine, multiple sclerosis, chemo induced nausea, etc
It can become rather automaton work. But it suits me. I only prescribe one type of drug and all my patients who see me know what they are getting. I still do get the weird patients who come and say they DO NOT WANT cannabis. usually it is cos a family member wants them to see the doctor to discuss. But I always go with the patients' wishes. If they dont want to take medical cannabis then don't.
I have likened my practice a but like running a Chicken on the Way. It is a friend chicken chain that only sells fried chicken and fries. Menu is more like how many piece of fried chicken you want rather than like those Chinese restaurants can have so many menus which are pages long. new promotion new menu new chef what not.
Simple lah.
- Joined
- Oct 7, 2012
- Messages
- 5,228
- Points
- 113
Eh don't insult lah. I am not a cannabis dispensing automaton.
I dispense nothing
I only write prescriptions. How many grams/day. And the grams/day is not really how much the patient uses. It is an authorization to how much they can buy.
The Federal Law for ACMPR when it started was to allow patients to be able to legally possess cannabis for medical purposes. Back then mostly people all carry dried flower or milled cannabis. So if they had 2g/day prescription, then it means they can at any time possess 30 day supply ie 60g. Police will weigh and see if below 60g.
These days medical patients use mostly oils. and every Licenced Producer (LP) has a conversion factor.
https://hmed.ca/oil-equivalency-jun-2019/
Eg most LPs would be able to produce 5-8 ml of CBD or THC oil from 1g of dried cannabis. When I explain to my patients I usually use the 1g = 8ml of oil So a 40ml bottle used 5g of dried cannabis to make. Hence if you have a prescription of 1g/day then you are allowed to buy 6 bottles of oil per month or a mix of oil and actual weight of dried flower.
Often we increase the prescription amount not because they actually use that much but because patients want to have more than one LP. Eg they might want to go with Spectrum Cannabis, Aurora Cannabis and Cannimed. Then we write 3g/day and send 1g/day to each of the 3 LPs.
Shoppers Drug Mart is an LP but they dont grow their own cannabis. Through their portal you have access to 12 differnt LPs. You dont get access to all the products in each LP under the SDM umbrella but at least you get more variety.
So there are various nuances in the medical cannabis market.
Patients dont get their prescriptions. We send it to the LPs they want to sign up with. The patient will go on the website and register. Then the LP sends a confirmation email back to them indicating they can order product. They put in orders online or over the phone pay using credit card and then the products are mailed to their address on file.
CPSA requires all physicians writing medical cannabis authorizations to see their patients for follow ups at minimum intervals of 3 months. This is the standard of practice. So every patient has to see the doctor at least 4 times a year.
Since legalization the number of patients wanting prescriptions has dropped considerably since you can just walk to the recreational store and get THC CBD and what not.
Hence the practice of medical cannabis now is very much made up of genuine patients who require help with anxiety, insomnia, chronic pain (top 3 conditions). We do get the GI patients eg IBS IBD, Celiac, migraine, multiple sclerosis, chemo induced nausea, etc
It can become rather automaton work. But it suits me. I only prescribe one type of drug and all my patients who see me know what they are getting. I still do get the weird patients who come and say they DO NOT WANT cannabis. usually it is cos a family member wants them to see the doctor to discuss. But I always go with the patients' wishes. If they dont want to take medical cannabis then don't.
I have likened my practice a but like running a Chicken on the Way. It is a friend chicken chain that only sells fried chicken and fries. Menu is more like how many piece of fried chicken you want rather than like those Chinese restaurants can have so many menus which are pages long. new promotion new menu new chef what not.
Simple lah.
No time to waste on pharmacy dispensers who fancy themselves to be something else ...
No time to waste on pharmacy dispensers who fancy themselves to be something else ...
I write. Is up to you to read of course.
Relax lah bro. I mean you no harm.
I am pretty consistent. I have no malice against individual bros here in SBF or even individuals in sinkieland.
But I hate sinkieland in general and the 70%!
So anyone here who get offended when I curse SG and sinkies please hor.....don't get offended unless you consider yourself one of the 70%!
- Joined
- Oct 7, 2012
- Messages
- 5,228
- Points
- 113
I write. Is up to you to read of course.
Relax lah bro. I mean you no harm.
I am pretty consistent. I have no malice against individual bros here in SBF or even individuals in sinkieland.
But I hate sinkieland in general and the 70%!
So anyone here who get offended when I curse SG and sinkies please hor.....don't get offended unless you consider yourself one of the 70%!
I don’t waste my time with pharmacy dispensers masquerading as docs. BTW, did not even bother to glance at much less read your last two posts. You obviously are a loser who blames others for your troubles, hate this hate that, blah, blah, blah. Lots of foreigners go to Mt E to consult specialists while they are in SG for other purposes - you MORON. They didn’t teach critical thinking skills in NUS med school, just need to memorise this and that? You can take the Sinkie of Sinkieland, but you can’t take the Sinkie out of him. You are confirmed and chopped not yet Unsinkified. That’s how you ended up being a glorified pharmacy dispenser.
- Joined
- Dec 6, 2012
- Messages
- 28,963
- Points
- 113
Eh KNN my uncle think he is KNNI don’t waste my time with pharmacy dispensers masquerading as docs.
I don’t waste my time with pharmacy dispensers masquerading as docs. BTW, did not even bother to glance at much less read your last two posts. You obviously are a loser who blames others for your troubles, hate this hate that, blah, blah, blah. Lots of foreigners go to Mt E to consult specialists while they are in SG for other purposes - you MORON. They didn’t teach critical thinking skills in NUS med school, just need to memorise this and that? You can take the Sinkie of Sinkieland, but you can’t take the Sinkie out of him. You are confirmed and chopped not yet Unsinkified. That’s how you ended up being a glorified pharmacy dispenser.
Aiyah of course it is possible you go to sinkieland for medical tourism lah.
But if you are aussie why waste money going to Mt E? Aussie healthcare so bad meh?
And SGD$450! geez! If they didnt do a TURP (and I suspect they did not for that low price) you kena cheated lah!
Flomax and Avodart doesnt cost so much!
Maybe you have bladder cancer? And needed BCG infusion into bladder?
Chill lah.
Anyway I got my licence. I can choose to do wahtever kind of medicine lah
Eh KNN my uncle think he is KNN
View attachment 74842
sweetiepie you also angry with me ar
I mean you and your uncle no malice ok?
- Joined
- Dec 6, 2012
- Messages
- 28,963
- Points
- 113
In case you never watch this before KNN the cast suit your cast here KNNsweetiepie you also angry with me ar
I mean you and your uncle no malice ok?
Since dropping out from the medical school, Lau Mack has been living a humble but contented life, running a small clinic in a shabby area, treating local inhabitants and poor prostitutes working there. One night, he escorts an injured gun robber to the government hospital, where he unexpectedly meets his old friend from college time, Dr. Jaw, now a reputed surgeon with an aspiration for senior management. To Jaw’s bitter surprise, he finds himself outshone by Lau’s medical talent and kindness to patients. Jaw is however determined to speed up his career ascent at the expense of Lau. His plots work perfectly, until an accident delivers his life to the mercy of Lau.
Tony Leung as the happy-go-lucky Lau Mack, the eponymous doctor who’s oft lauded as the best surgeon in Hong Kong but at the same time vilified by the medical board for his questionable ethical principles. A pariah in the medical community, Mack strikes out on his own and runs a small clinic in a troubled neighborhood—with prostitutes, hoodlums, and other oddball types making up his regular clientele, and so lots of dirty and irreverent jokes abound
- Joined
- Jul 15, 2008
- Messages
- 22,294
- Points
- 113
Can't help but notice his snidey commentary posts all over forum of late. For a canuck MO, he's keeping some odd hours hereU have all the kaypohchee and fake characteristics and behaviour of that moron screwed ball. Whether I are same or different person is besides the point. Go back to your dream of being a cannabis dispensing automaton.

Similar threads
- Replies
- 25
- Views
- 2K
- Replies
- 0
- Views
- 166
- Replies
- 5
- Views
- 717